
Score-3 Lesions: What to do with them? To biopsy or not to biopsy? Two easily assessable parameters may help with the decision.
/
J Magn Reson Imaging. 2016 Feb;43(2):325-32. PubMed PMID: 26131965
Short summary
An ADC-threshold and previous biopsy history are proposed to select Likert-3 lesions "benefiting from biopsy".
Conclusion
- Men without prior negative biopsy: ADC metrics helped detect GS>6 tumors.
- Men with prior negative biopsy: Biopsy in Likert-3 Lesions may be deferred due to the low frequency (2%) of GS>6 tumor found.
- ADC-threshold showed better specificity in guiding biopsy decisions in Score-3 lesions than PSA.
Patient cohort
Retrospective assessment of 158 men with Likert-3 lesions.
The New and the Good
- Two easily obtainable parameters, one quantitative (ADC) and one from patient history (biopsy history) are being consulted to triage score-3 lesions.
- Sophisticated method of ADC evaluation (whole lesion analysis and histogram).
Limitations
- Whole-lesion ADC metrics are time consuming in daily clinical practice and require dedicated software. However, ADC mean - which is easily determined in daily image evaluation and shows high reproducibility - was associated with GS>6 tumor as well.
- Likert-scale not PIRADS.
- Single reader assigning Likert-scores.
- MRI/TRUS fusion biopsy instead of whole-mount prostatectomy specimens as histological standard of reference.
Possible consequences for clinical practice
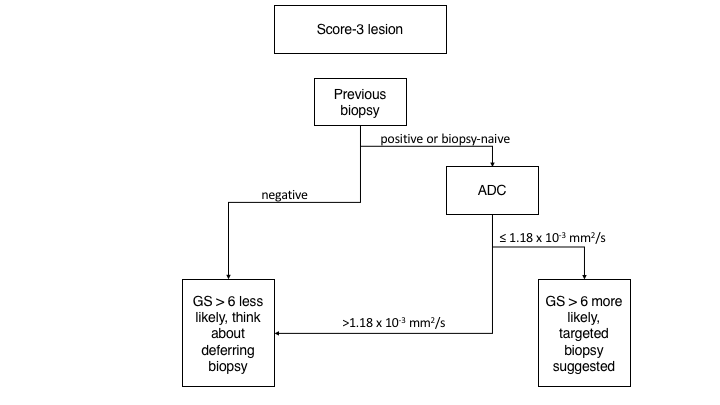
- If asked by the responsible urologist whether or not he/she should biopsy a score-3 lesion, an algorithm like this may be consulted to help the referring surgeon:
Possible implications for PIRADS v3
- Biopsy history may be consulted and implemented to triage PIRADS-3 lesions, e.g.:
- Previous positive biopsy or biopsy-naive → refer to biopsy
- Previous negative biopsy → biopsy may be deferred.
- In the former biopsy-group, quantification of ADC may become a "tie-braker" for PIRADS-3 lesions, e.g.:
- ADC ≤ 1.18 x 10-3 mm2/s → refer to biopsy
- ADC > 1.18 x 10-3 mm2/s → biopsy may be deferred to to small likelihood of GS>6 prostate cancer.
Future study ideas derived from this paper
- The proposed algorithms and results are preliminary and not yet validated. This question should be evaluated in a multicenter- / multi-system study to address the problem with ADC reproducibility among MR systems from different vendors.
Personal comment
- As I am always dissatisfied if I have to give a PIRADS score of 3, this study may help me triage those lesions into the "up for biopsy" versus "don't touch but follow" category.